A place to seek clarity on timeless issues and issues of the day.
Author: Harvey Cody
I'm a guy who has been told his perspectives and takes on things are interesting enough to deserve a blog. I'm humbled by the suggestion and have no particular reason to believe that many will agree with what I have been told. By no means do I claim my views capture ultimate truth or ultimate good. I hope that by reading what I have to say, you get closer to what you believe is true and good, or, at least, cause you to more carefully examine what you believe to be true and good.
The goal of “The Real Issues Concerning COVID-19” series of posts has been to sort out the real issues that will determine when and how economies will reopen in an economically effective and reasonably safe way. I’ve been frustrated that the information broadcasted by the Heath Experts Advising Politicians and The Public (“HEAPPAs”) has (1) caused too many people are too scared to begin to consider when and how to ease nonpharmaceutical interventions (“NPI”), (2) used incorrect and misleading data, and (3) generally failed to advise the public concerning the real COVID-19-related issues facing the American people. HEAPPAs sowed confusion rather than clarity. Confusion fostered doubt that stymies the adoption of useful strategies to move forward.
Having ushered the country into NPI strategy without an exit strategy, HEAPPAs owed the American people useful advice on how to get out of the mess they created. Instead, the little guidance they offered was typically impractical or uselessly sketchy.
Examples include:
HEAPPAs, without explanation, moved the goalposts concerning the purpose of “flattening the curve.” At first, it was to prevent hospitals from being overwhelmed. Then it was a general-purpose means “to save lives.” Their explanations concerning the first were clear and sound. The reasons concerning how lives would be saved by “flattening the curve” in the absence of hospitals being overwhelmed were virtually non-existent. Their failure to respond to credible critiques of “flattening the curve” being a general purpose life saver by many respected epidemiologist and others left the impression that HEAPPAs could not defend their position or were motivated by non-health objectives.
HEAPPAs have been mostly mum about the mental and physical harm and death inflicted by NPI — information essential to reasonable decisions about the costs and benefits of reopening. HEAPPAs ignoring their responsibilities to inform on these critical health issues have added unhealthy angst, stress, and discord to an already tum situation.
After months of silence on the subject, Dr. Fauci’s recently said[i] that he “totally supports” easing NPI because longer lockdowns could do “irreparable damage” to local economies. (Note: He couches the issue in terms of health vs. money, i.e., he talks about the thing about which he has no particular expertise and is silent on the negative health consequences of NPI). Then, he neutered the comment by adding “in a proper way in the appropriate setting,” without providing details concerning what way is proper and what setting might be appropriate.
The CDC adds to the messy messaging by publishing reopening strategies that are impractical.[ii] While Dr. Fauci’s and the CDC’s lips are saying “carefully reopen,” the practical effect of their words is “remain closed” — without explaining why staying closed is better than reopening. In other words, they have not explained why delaying the COVID-19 deaths is with measures that are killing people is the right approach.
Politicians and the public desperately needed information and constructive advice to make informed decisions and to get the required buy-in by the public so that customers and suppliers would be willing to engage in commerce. They have gotten roughly squat from the HEAPPAs.
As I’ve mentioned before, respected epidemiologists, who were not HEAPPAs (although some have testified to Congress), have disagreed with leaving NPI entirely in place.[iii] Yet, to my knowledge, until a few days ago, no one has advanced a concrete proposal as to how to proceed. Dr. Katz came close on May 7 but did not pull the trigger.[iv] A few days ago, Dr. Darria Long and Dr. David L. Katz came through with a sound framework, which, hopefully, will soon become the basis of a strategic plan.
[ii] For example, see “Considerations for Schools.” How can enough busses be built, bought, and delivered between now and the start of school to achieve 6’ spacing, i.e., two kids per row and only odd or even rows are available. That means that only 14 kids per trip can be transported in a bus designed for 39 kids. Will the kids in the bus at the back of the long que of busses get to the school house door before first period is over?
Before states started easing non-pharmaceutical interventions (“NPI”) to “reopen” their economies, misguided, but empathetic prophets of doom (“Doomsters”) gnashed teeth, wailed, and jeered those who they thought were enabling COVID-19 to slaughter people for the sake of money, leisure, spite, or political gain. They declared that easing NPI would cause spikes in deaths. They never bothered to provide theories as to how slowing the spread of the virus might decrease the ultimate number of infections, much less how such slowing could save lives during times when no hospitals were at risk of being overwhelmed. Neither did they offer data showing that carefully easing NPI would cause the ultimate number of COVID-19 deaths to be higher. Instead, they validated their beliefs only with assertions, mantras, and chants and ignored the deaths and damage to physical, mental, and fiscal health inflicted by NPI.[i] (Sadly and irresponsibly, the people advising politicians and the public neither validated nor refuted the Doomsters’ claims — but that is the subject of a future blog post.)
Though epidemiologists who speak from government podiums have not weighed in on the Doomsters’ claims, all epidemiologists assure us that the truth is in “the data.” So, let’s look at how Doomsters’ claims fare in light of data on how the epidemic has played out in Texas before and after NPI easing.
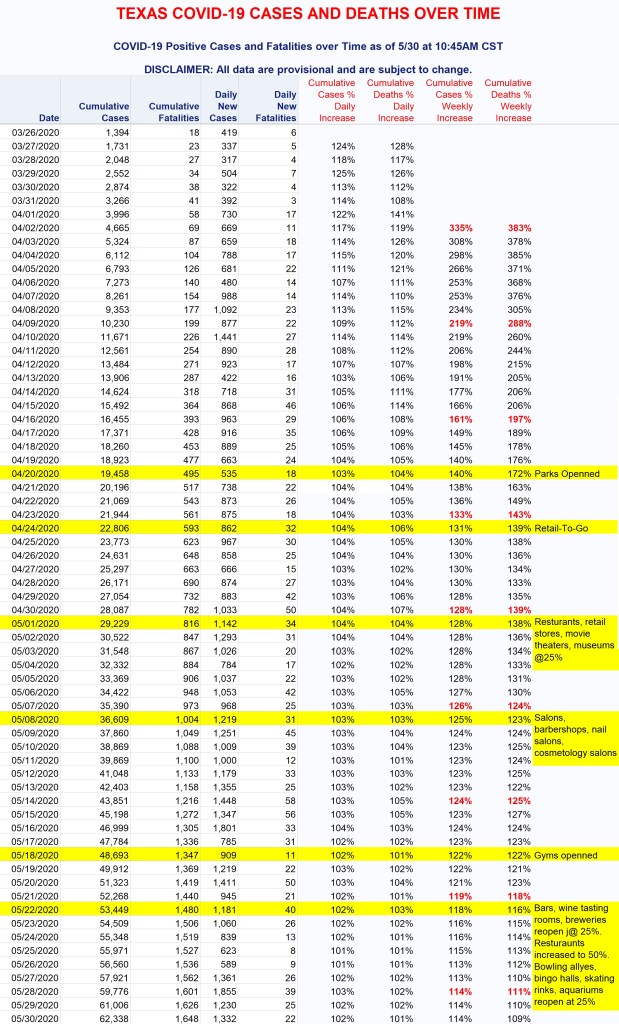
Texas’s first confirmed COVID-19 death occurred on March 15. Dallas/Ft. Worth officials ordered some business closures on March 16. “Shelter-in-place” orders for Dallas and Houston came on the 22nd and 24th, respectively, when just a few COVID deaths had occurred in Texas.[ii] Texas’s COVID-19 dashboard started on March 26. (That dashboard has all the problems I previously described the COVID Map[iii] has plus some others,[iv] but it is the best available information.)
Interesting items revealed by the above data include: Texas’s daily confirmed infections at the end of the first were 3.35 times the rate on the first day. Deaths were 3.83 times higher. At the start of the epidemic, COVID-19 was rapidly expanding. Note also that from the end of the first week, both rates have steadily declined. The confirmed cases and deaths on May 30 were only 1.14 and 1.1 times higher than the week before. Until May 5, the percentage increases in deaths were consistently higher than the increases in infections. Since then, the opposite has been the trend.
What is most striking, however, is that when Texas began reopening on April 20, the increase in infections was 4% per day. Forty-two days and six phases of NPI easing later, the rate of growth had fallen to 1% for a week. During that time, Texans progressively relaxed their NPI practices more than recommended by NPI guidelines, and some people abandoned NPI altogether. In short, despite the progressively greater social interaction since NPI started easing, the rates of infections and deaths have fallen steadily. There is reason to believe that the reported daily infection rate will soon show falling rates of infections despite increased easing.[v]
In reality (as opposed to the reported numbers), if it were not for the significant increases in antibody testing in May.[vi] Part of the increase in confirmed cases was due to testing more people in the later period. In other words, in reality, Texas’s daily infections are likely falling rapidly right now. The Doomsaying has been debunked by the data!
What is especially remarkable about this news is that, while NPI has proven to be mostly ineffective in protecting the vulnerable (despite politicians solemnly swearing to protect them), progress toward herd immunity has advanced while infection rate increases have fallen. Wherever tried, reopening economies will hasten the day herd immunity is achieved. That will be the day people will be less scared to engage in normal commerce, and vulnerable people can finally breathe easy and be comfortable around their loved ones.
That the Doomsters vehemently continue to insist that not following NPI will cause more ultimate deaths makes clear they have been relying on emotions rather than data and analysis. To their great discredit, epidemic experts who have commanded the stage and bathed in its limelight have neither validated Doomsters’ declarations nor clarified what is wrong with them. Rather than debate the epidemiologists and others who do point out the errors in the Doomsters’ thinking, they stand idly by as YouTube, Facebook, etc. takedown contradictory content. (That they prefer silence to losing the debate is a fair assumption.)
Doomsters’ claims fly in the face of the too few experts who are brave enough and willing to counter the established groupspeak on these subjects. For example, Yale’s Dr. David Katz[vii] says, “If all we do is flatten the curve you don’t prevent deaths, it simply changes the date of their death.” Variations on that theme have been provided by Dr. John Ioannidis,[viii] Knut Wittkowski[ix] and Professor Johan Giesecke,[x] Professor Sunetra Gupta,[xi] and others.[xii] As the Doomsters shouted, “Wear a mask, save lives,” the data and many responsible experts are saying calmly and convincingly that the Doomsters do not know much about what they are wailing (while Dr. Fauci or Dr. Birx remain mostly mum on the subject).
The Doomsters’ “thinking” did include a true factoid. Until the virus fades out, increases in social interaction/contact will cause the rate of infections to be higher than would otherwise be the case — at least for a while. Easing NPI increases social interaction/contact. Increased social contact causes increased infections until a high enough percentage of the people interacting are immune to the virus, i.e., when herd immunity is near or achieved.
Unless a sound argument that NPIs still saving lives is made, worrying about increased infections is misplaced. It is like fearing that a bucket will drain faster if a hole in its bottom were enlarged. The same amount of water will leak out regardless of the rate at which the water leaves the bucket. The only sure way to drain COVID-19 from the environment is for the population to achieve herd immunity. Delaying easing is delaying the inevitable number of infections that are needed to achieve herd immunity will ultimately save no lives. However, NPI will ring up deaths until eased out of existence.
When fears of hospitals being overwhelmed, insufficient medical supplies being available, and/or doctors needed time to discover how to diagnose and treat the new virus, “lockdowns” may have been justified, i.e., the damage from “lockdowns” might have been less than the damage the lockdowns were inflicting while those problems persisted. Now that those reasons for aggressive NPI no longer apply, ignoring the compounding damage NPI designed for bygone concerns inflicts is irrational. By ignoring the damage NPI inflicts, Doomsters are blind to the goal the ultimate goal of epidemiology, “draining” the environment of COVID-19 as quickly as possible without overwhelming the healthcare system.
As is so often the case, Doomsters are harming (killing, sickening, weakening, and otherwise ruining lives of) people they believe they are helping.
Joe Biden telling some blacks, “you ain’t black,” tells much about Joe Biden.
Let’s set aside the arrogance of Biden’s presumption that he has the privilege to judge who is and isn’t black. Instead, let’s sort out the embedded bigotry and self-interest revealed by Biden’s comment.
Having once been one, I can confirm with confidence that most Democrats would prefer not to entrap black people into government dependency. They have a sincere desire for blacks to thrive and believe they have the innate wherewith all to do so. (BTW: Though most Democrats seem to deny or doubt it, the same is true of all but a tiny and impotent fraction of white people.) Sadly, however, they vote for people like Biden, who consider entrapping blacks in poverty is a small price to pay to gain the fame, fortune, and power they seek.
Pursuing his self-interest over the public interests, however, is not the worst of Biden’s failings. Biden epitomizes the kind of people infused with what Bush II called “the soft bigotry of low expectations” for blacks (and certain other minorities). In general, they presume that blacks lack the innate capacity to think, provide, or make sound choices for themselves. These people, who are afflicted with a savior complex,[i] believe that blacks could not make it without them. (That belief is demonstratively false.[ii]) Blinded by the vainglory of being a savior, they do not see the quixotic damage they inflict on the people they believe they are saving. Ironically, they do not realize that the reason so many blacks do not provide or make sound choices for themselves is that the white saviors prevent too many of them from going to schools that will teach them to do those thing while telling them that learning isn’t important because the system is so rigged against them that no amount of learning would do them any good. (Pay no attention to the 35,000 black millionaires in America and the legions of middle and upper-middle-income blacks?) Even if it were true, which is is not, that messaging alone would discourage many blacks not to try. Many, if not most, who would have tried absent that messaging would have succeeded.
Biden’s comment reveals his belief that blacks who can think for themselves and reach conclusions different from the majority of people with a similar hue are so different from blacks that they belong to a different race. (Note that Biden would never believe or say those things about whites or some other races.) Biden’s only slightly veiled presumption is that blacks cannot think for themselves, and, therefore, should not be permitted to have the freedom of thought that other, he presumes more capable races have and should have. It’s disgusting.
Biden and other Democrats are telling blacks that if blacks step out of the self-destructive boxes constructed for them by white politicians (and blacks who make a living or gain power by supporting those politicians), they will be disparaged and exiled from their race. People of all hues should condemn that malignant, discouraging, and disabling messaging to blacks. If, however, the vast majority of blacks continue to accept that dehumanizing message, LBJ will be proven to have been a perceptive, cunning, and ruthless politician willing to sacrifice the futures of many blacks to retain power for Democrats “for 200 years.”[iii]
Yet, there are signs that many blacks are catching on to the false promises of politicians like Biden. The Blexit Movement is a growing force in America. Hopefully, Candace Owen’s, Larry Elder, and similar efforts to free blacks from the bondage of Democrat party will be successful.
[i] “The White-Savior Industrial Complex.” A slice of Teju Cole’s insightful piece, “What innocent heroes don’t always understand is that they play a useful role for people who have much more cynical motives.” White savior’s beliefes and attitudes toward problems in Africa are quite similar to their beliefs and attitudes toward problems in poor black neighborhoods.
On May 15, 2020, Russ Roberts published another splendid podcast interview of Paul Romer, “economist and policy entrepreneur, is a co-recipient of the 2018 Nobel Prize in Economics Sciences and University Professor in Economics at NYU,” and more.[i] The podcast focused on several aspects of the COVID-19 pandemic. While I highly recommend that you listen to it, Romer adding his mallet to the drumbeat for widespread testing advocates is unhelpful.
Widespread testing (“testing”[1]) was among the podcast’s topics. According to Romer, testing is the key to getting people comfortable enough to actively engage in commerce—which both Roberts and Romer believe to be of paramount importance. Enough people being that comfortable is essential to any semblance of a recovery. His “case” for how and why testing would accomplish that goal was this:
“The idea with testing, though, is that if there’s some information we don’t have, what we’d like to know is whose infectious right now. If we knew that information, what we could do is say we’re going to isolate those people for a short period of time, a few weeks, and we can then suppress the virus without interfering with anybody else’s daily lives.”
Note, however, that “case” does not identify either how or why testing should or will cause people to be more comfortable.
Other advocates of testing offer different rationales:
Dr. Fauci: “The one thing we hopefully would have in place, and I believe we will have in place, is a much more robust system to be able to identify someone who’s infected, isolate them and then do contact tracing.”[ii]
CDC: “CDC has a strategy for using antibody testing as part of surveillance efforts to better understand how much of the U.S. population has been infected with SARS-CoV-2 and how the virus is spreading through the population over time.”[iii]
WHO: “identify, isolate and contact trace people with the disease,” “vital part of understanding the scale of the outbreak and how it is evolving” and “Effective testing and quarantine measures help ease the pressure on health services, which can quickly become overwhelmed as demand surges for respirators and other critical lifesaving equipment.”[iv]
The Media: The media doesn’t even try to explain testing’s goal other than identifying hotspots (which happened without testing) or whether tracing could be effectively and acceptably implemented.[v]
Those rationales aim to slow or stop the virus’ spread, i.e., “flatten the curve” or some unidentified way to permanently stop the virus from infecting people. They offer no insight as to how testing is a substitute for herd immunity to stop the pandemic. Tinkering with the timing of when the virus infects and kills is of great value only when hospitals are at risk of being overwhelmed. Otherwise, “If all we do is flatten the curve you don’t prevent deaths, it simply changes the date of their death,”[vi] Time is not on the side of the especially vulnerable.[vii] Rarely do people believe that fiddling while Rome burns is a good strategy—but here we are.
Let’s sort that out why testing and tracing are impractical and inapplicable to America.
One of the goals of testing is to enable “contact tracing,” i.e., find someone infected, identify everyone the infected person encountered, and whisk them all away to confinement. For sake of argument, let’s assume that the needed infrastructure (wireless surveillance, electronic notification systems, human catchers, detention centers, staff, and supply chains, courthouses to try habeas corpus cases, etc. and popular acceptance and adoption thereof) could be in place and running smoothly before the economy collapses. Is that the society in which we want to live? By forcing people to wear ankle bracelets and accept detention, S. Korea[viii] pulled it off, as did China by forcibly removing people from homes and throwing them into coronavirus detention facilities.[ix] Americans will not go there peaceably.
America tried a milder version of contact tracing. Here is what Romer said about that:
“…[America’s early attempts at contract tracing] partly colored by our experience, which was: the contact tracing system was the system we were using in January when this virus exploded, and it just completely failed. The people who say, ‘Okay, well contact tracing is going to work, give us a do-over,’ I don’t see the evidence that it’s going to be different if we do it again.”
Consider the practicality of widespread tracing. America’s population is about 325 million. People are spread across and between 35,000 cities and towns. Consider the following variables to be normalized in order to make sense of COVID-19 test results concerning how many people are infected; have become immune, seriously ill, and/or died:
What are the mixes of preexisting conditions, age, race, and abilities/willingness to follow protocols;
What protocols were established, when, and how aggressively; and
Which local politicians/officials were smart (the jury is still out on this) or dumb[x] in their speeches and policies; and
What other variables play a role, e.g., temperature, humidity, and sunlight.
Each of these variables varies significantly from place to place. For example, compare COVID-19’s impact on the comparably sized populations of New York State and Florida. As of 5/17/2020, confirmed cases were 350,121, and 45,588 and deaths were 22,478, and 1973. The pandemic will have run its course before all the significant variables are identified and quantified sufficiently to be actionable.
Consequently, sampling must be done on a granular level to be useful. Collecting, analyzing, and applying that much data effectively is too massive to be accomplished. For example, if an average of 2000 tests were taken in 35,000 towns (forgetting about all the places in between), 70 million tests must be taken, shipped to labs, and analyzed per round to obtain the needed information. However, both diagnostic and serological tests are required. So, 140 million tests would be necessary. At 770,000 tests per day, America is leading the world in the number of tests per day. That is about 0.5% of the tests needed per round.
Consider how often test rounds are needed. Infected people typically shed high amounts of virus soon after infection and are asymptomatic for at least a few days. Irrespective of symptoms, people can be infectious for 10 days or more.[xi] Let’s say a person goes to a testing facility, and three days later learns the test was negative. However, she may have become infected when she pulled the handle of the facility’s exit door. She would soon start shedding COVID-19 for many days while believing that she is virus-free. “To be safe,” she should get tested every day until she finally tests positive or the pandemic has run its course. People are already not showing up at test sites.[xii] Because the virus can spread so quickly, the shelflife of test data is too short to be of much practical use—and getting close to enough tests everywhere is impossible.
For random sample testing to work, the people tested need to be representative of a larger group. Unlike randomly calling people, people who are willing and able to get tested could be very different from the larger group. People with no better way to earn money than getting tested will not be representative of the whole. People are already growing tired of being prevented from working, standing in breadlines, and staying at home. That sentiment is likely to increase until nonpharmaceutical interventions (“NPI”) stop. Will the data collected before a general abandonment of NPI be relevant when people have thrown off their masks and left the house? Will the people of all cities start abandoning NPI at the same time or the same rate? If not, most of the data collected will be of little practical use.
As noted above, tracing is for finding people to quarantine. However, as Dr. Jay Bhattacharya says, “That works fine if you have a small number of people who have been infected [which is not the case in the places where COVID-19 is a big problem] and… we’ve seen a very large number of people don’t have very many symptoms and, yet, can spread it, this kind of strategy will not work. It is doomed to fail. In fact, it’s going to be counterproductive to do a strategy like this… [if when they show positive, they will be quarantined] people will say they don’t want to be tested.”[xiii] To be effective, quarantining must be enforced. Believing that forced testing/quarantining would work outside an authoritarian state is likely irrational, but certainly would produce unrepresentative/invalid test results.
Romer suggests that problems with quarantining might be solved by the government paying people to be quarantined. There are people on whom that might work and others on whom it will not, e.g., Jeff Bazos or the owner of a successful restaurant. The disparate results of randomly testing/quarantining poorer people is not a compelling strategy.
When pressed on how test results would be used, Romer said, “it’s premature to worry too much about what we do with that information.” He also made some of the “arguments” discussed above. However, they have the failings discussed above.
If there were a good argument for testing, surely Paul Romer and many other testing advocates would know what it is and would have already widely disseminated it. I’ve looked in vain for a sound argument.
On the off chance, a credible case for widespread testing exists, epidemiologists owe the public:
a clear presentation of the case,
an explanation as to why delaying the spread of the virus is not merely putting off the inevitable deaths that COVID-19 will cause.[xiv] and
an identification of the point at which NPI will cause more illness and death than COVID-19 will (to say nothing of the lost dignity, security, thriving, and fun being destroyed by NPI).[xv]
Absent that: The public should reject the claim that NPI easing must await widespread testing.
Let’s hope that people will soon realize the impractically and inapplicably of the testing “solution.”[xvi]
_________________________________
[1] Unless the context in which the word, “testing” is used is talking about individual testing for nonepidemiological reasons, “testing” refers to widespread testing.
Whether one should wear a mask us a multifaceted issue. This post will address only two of them
I’ve seen posts in which people say that masks do no good. That is wrong. They do both good and bad.
Many seem to base their claim on the fact that the holes in masks through which air passes are larger than COVID-19 molecules, i.e., molecules come through to the wearer and go out to possibly infect other people.
While that factoid is true, the area of masks is mostly material. COVID-19 molecules and saliva teeming with COVID-19 get caught on the inside and outside of the mask. So, masks stop some of an infected person’s shedding of COVID-19 molecules (and wearing a mask does not prevent COVID-19 molecules from getting to the wearer).
On the other hand, “viral load” is a very big deal. Each COVID-19 molecule that enters a body starts multiplying. As soon as a well functioning immune system detects the presence of the virus, it starts fighting the virus, including producing antibodies against the intruder. Each antibody can kill only one COVID-19 molecule. How ill a person becomes very much depends on whether the pace of the body’s antibody production exceeds the pace at which the virus is reproducing.
A person’s immune system is much more likely to outpace the virus if the “load” that enters a person’s body is a single COVID-19 molecule (as opposed to say, a person at the peak of their viral infection coughs in the face of the person at the same moment they happen to be taking in a deep breath. An immune system trying to outpace many thousands of multiplying COVID-19 molecules is less likely to catch up before it is too late.
The flip side is that one of the body’s ways of fighting the virus is to eject them by coughing. If the virus gets caught in a wearer’s mask, some of the molecules will go right back to where they came from each time the mask wearer breaths in. Once back in the body, those recycled molecules will continue to replicate.
_______________________________________________
ADDENDUM: Shortly after I published this post I ran across THIS VIDEO. I haven’t verified the extent to which it is true, but there is reason to believe that it is not entirely false.
Discussing anything positive about COVID-19 amid the heartbreaking tragedies it has wrought will understandably be considered to be perverse by many. Letting that perversity prevent the good news spreading and calming fears is counterproductive. People need to be fully informed to make sound decisions about how to proceed. Closing one’s eyes to the light at the end of the tunnel is not helpful.
We hear, “COVID-19 is a unique virus” frequently. That statement is true but insipid (all viruses are unique ). Some of COVID-19’s quirks are especially bad, and others are especially helpful to the task of easing nonpharmaceutical interventions (“NPI”) to improve health outcomes and get the economy turned back in the right direction. Sooner is better than later. Let’s sort some of those out.
The Good News About Covid-19
A Selective Savage.
The Victims. COVID-19 is unusually selective concerning which groups it severely affects or kills.[i] While we would prefer that it killed no one, a virus that slaughters children and young adults in the prime of their lives would be devastatingly worse than COVID-19. The death of an aged parent fraught with medical problems and much nearer death than their progeny is sad but is often coupled with relief that suffering has come to an end. Additionally, most parents would prefer to trade their lives to save the lives of any of their children or grandchildren, to say nothing of multiple children and grandchildren.
The average age of people killed by COVID-19 in Massachusetts as of 4/22/2020 was 82.
Of all fatal cases in New York State, two-thirds were in patients over 70 years of age; more than 95 percent were over 50 years of age; and about 90 percent of all fatal cases had an underlying illness.”[ii] Data from New York City on 4/18/2020 indeed is not entirely representative of everywhere in the US, but it is nevertheless telling as to how the virus discriminates by age.
For people 20 – 65, the risk of having severe symptoms from the virus is approximately 80 times lower than for people 75+,[iii]e., the risk is negligible.
The Spared Many. While exceptions[iv] to the rule that COVID-19 spares harm to virtually everyone younger than 21. With the possible exception of NYC, the risk of adults dying from COVID-19 is about the same as the risk of getting hurt driving on highways of a congested city for several hours.[v] Dangerous, but not a reason to upend everything.
With or without a preexisting condition, an American under 65 is 15 times less likely to die than a person over 65.[vi] For an American under 65 with no preexisting conditions,[vii] the risk of death from COVID-19 is negligible.[viii]
This reality creates an opportunity to deploy reopening plans that attempts to protect the exceptionally vulnerable (something NPI is failing to do[ix]) while enabling people with a slight risk of COVID-19 complications to get on with their lives and engage in much-needed commerce.
♦ The country has many more palatable options to ease NPI than would have been expected had COVID-19 pandemic been as predicted.
Who Needs Protection. Preexisting conditions are a considerable part of the COVID-19 story. COVID-19 is much more lethal to people with certain known preexisting conditions[x] than most cases of flu and kills a somewhat higher percentage of cases. As of April 10, when 96,000 people had died of COVID-19, less than 1% of them did not also have one or more comorbidities.[xi] As you can see from the chart below, the risk of death from COVID-19 in the absence of a preexisting condition is remarkably low. For example, the percentages of people 65-74 years old and 75+ years old who die of COVID-19 with no known preexisting conditions are 1.5% and 0.8%, respectively. Stated differently, 97.7% of the people over 64 years old with no preexisting conditions survive a COVID-19 infection. Of those people whose preexisting conditions were unknown, the vast majority likely had preexisting conditions.
♦ We know who needs to stay at home, social distance, wash hands, etc. in order to save lives;
♦ We know who need not distance themselves from people similar to themselves;
♦ The additional COVID-19 risks to the 65+ crowd are almost exclusively about their preexisting conditions that put them at risk of death from COVID-19. The threat to healthy 65+ people is very low, and
♦ The exceptionally vulnerable people are disproportionally dying in the first (and hopefully only) wave of the virus. Conversely, the population that has yet to be infected is likely to be less likely to die than during the first wave.[xii]
The Data Used To Devise NPI Strategies Was Flawed.
As discussed in “It Was “the data,” the “Confirmed Cases” of COVID-19 used to devise the NPI strategy understated the number of infections in countries. COVID-19 death rates are the number of deaths caused by the virus divided by the number of people infected. When the number of infections in the denominator is too low, the death rate is overstated. (More validation of the claims in “It Was “the data” have come in.[xiii]) The US NPI strategy adopted to deal with a pandemic relied on an early Imperial College London model death That model depended on an understated denominator and lies[xiv] about the virus coming from China. TheICL model estimated that COVID-19 would kill 2-3% of infected people and 2.2 million Americans.[xv] The low end of its range is 100 times more than now expected.
Consequently, America’s NPI strategies assumed a pandemic 150 times as deadly as COVID-19 turned out to be. So, US NPI was significantly more aggressive than was necessary or appropriate—even in the nation’s hottest hotspots.[xvi] They were wildly more aggressive than were needed everywhere else in the country.
“Given the positive correlation between population density and influenza mortalities, cities are likely to have greater mortality rates than rural areas.”[xvii] Consequently, imposing, NPI appropriate for major cities in most states was based on fear, not facts and science. Universally applying that NPI anywhere for more than two or three weeks was unwarranted, if not absurd.
♦ COVID-19 is not nearly as deadly as the public has been led to believe.
♦ Easing of NPI designed for a much more deadly virus that COVID-19 is appropriate everywhere.
♦ Decisions not to ease off NPI that proved to be over-aggressive are neither data-driven nor scientific—although reinstituting some NPI in the unlikely event that a hospital becomes at risk of being overwhelmed might be necessary.
Antibody tests cannot be perfect, i.e., sometimes they produce false positives or false negatives. Not wanting to record or tell people that they are immune when they are not, antibody tests are designed to err on the side of producing false negatives.[xx] Consequently, more people have immunity than antibody testings suggest.
♦ We have an unexpected jump start on reaching herd immunity. A goodly percentage of people can neither spread the virus nor be harmed by it.
♦ The likelihood of people becoming infected today is lower than the probability of becoming infected was when the outbreak started.
♦ Most important, the nation’s vulnerable people are less likely to become infected now than they were when the outbreak began, i.e., the likelihood that the virus can avoid the multiple dead-end paths that prevent the virus from landing on vulnerable citizens has fallen significantly.
Many more pieces of good news could be chronicled. However, once honed by marketing professionals, the good news described above could empower the mainstream messengers to calm the unwarranted fears of healthy young people that are needlessly preventing them from reasonably safely getting on with their lives, and thereby increase protection of the vulnerable and get the economy turned in the right direction.
Let’s do what we can to get this good news message to the public.
[1] Dr. Birx and others have mentioned they do not have data to prove that COVID-19 infections confer immunity, but neither do they have data or analysis to confirm that the virus does not confer immunity. The possibility that it does not is unlikely.[1]
[iv] Until recently there were no remarkable exceptions concerning children. Recently (months into the pandemic), some concern about a possible association between COVID-19 and Kawasaki disease in children has arisen. “Kawasaki disease is a very rare, but treatable, condition that causes inflammation in blood vessels, and toxic shock syndrome is a life-threatening bacterial infection.” While “Three New York Children Have Now Died from Mysterious Illness Linked to Coronavirus,” the motivations of those who are making the link and why the link is made to COVID-19 is an important issue. How do they explain (1) why some children with the disease have not tested positive for either the virus or COVID-19 antibodies, and (2) why the disease is an issue in so few countries. In addition, it is likely to be a very long time before proof that the bacterial infection is not due to NPI deployed to fight the infection on account of being couped up in the relataively sterile envoroments rather than the virusCOVID-19. Right now, there is no science to say that the virus is even the likely culprit.
See, “15 Children Are Hospitalized With Mysterious Illness Possibly Tied to Covid-19” and
Author’s Note: This post presents what I believe to be logical extensions of claims made by the epidemiologists, virologists, and statisticians herein cited. They appear to me to be very authoritative. Not having expertise in those fields, I cannot certify their accuracy, and my interpretation of what they said could be faulty. Nevertheless, if those experts and my interpretations and analysis are correct, the following discussion is critical in our efforts to protect the vulnerable and minimize economic damage from COVID-19. Spoiler alert, it is very different from the mainstream narrative.
🙛
Let’s sort out some of the problems concerning the mainstream messaging about COVID-19 that causes the public to believe that rising numbers of infection is bad and that a steady or falling number of infections will lower the number of people who eventually die from COVID-19. That messaging is non-scientific and is slowing the rate at which the country can get back to business, which is counterproductive. Let’s call it “The Herd Immunity Messaging Problem.”
Society should do what can reasonably be done to protect the people who are likely to be seriously harmed or killed by COVID-19. As discussed in earlier posts and below, no countries are doing a good job of protecting those people. New York Governor Cuomo presented a chart of data collected over the most recent several days showing from where hospitalized people came.
As you can see, 66% of people had come from home and 12% came from nursing homes and assisted living facilities. Clearly, lockdowns are not foolproof and people are not safe at home. Yet the “STAY AT HOME” messaging that was devised based on what was feared about a virus the designers knew little. The designers who constantly say, “we need more data” are simultaneously confessing that their plan was not based on the needed data. Let’s sort out the problems with staying on message after contradicting data has been collected.
THE ULTIMATE GOAL OF NONPHARMACUTICAL INTERVENTIONS (“NPI”)
When no one in a population has been infected, the vast majority of people on whom the virus lands are vulnerable to infection. NPI (stay at home, protective gear, washing hands, etc.) lowers the odds of infection some, but far from completely. In the early stages of a pandemic, anyone infected will likely pass the virus on to multiple other people, each of whom will likely infect multiple other people. That process creates exponential growth of infection (“the wave”), a normal feature of pandemics. Not long after becoming infected, almost everyone becomes immune to the virus or dies.[i] However, as the immune share of a population increases, paths to vulnerable people become more blocked by immune people who will kill the virus instead of passing it on. If enough people get infected,[1] the odds the virus can find a path through the multiple blocked paths to a vulnerable person becomes slim that the virus can no longer find enough new victims to sustain itself. That level of infection in a population is called “herd immunity.”
“With all respiratory diseases, the only thing that stops the disease is herd immunity.”[ii] Consequently, achieving herd immunity should be the ultimate goal in the battle against COVID-19.[iii] The virus will continue to infect more people until herd immunity stops it. Perforce, any location that has not yet achieved herd immunity needs more infections. Yet the public has been led to believe that more infections are bad. Houston, We have a Herd Immunity Messaging Problem!
“Flattening the curve” has been a big part of the mainstream narrative. However, flattening the curve is not a tool to achieve herd immunity. On the contrary, it slows progress toward that ultimate goal. In theory, flattening the cure can save a few lives, but it also causes many problems, including serious illness and deaths. (See Part I, Part II, and PART III.) We are told to “listen to the experts,” but some epidemiologists say NPI will have little effect on the total COVID-19 deaths any country is destined to have,[iv] while others say the NPI in most places turned out to have been a huge mistake.[v]
Flattening the curve can help prevent hospitals from being overwhelmed. Otherwise, as Knut Wittkowski, previously the longtime head of the Department of Biostatistics, Epidemiology, and Research Design at the Rockefeller University in New York City, put it:
“[W]hat people are trying to do is flatten the curve. I don’t really know why. But, what happens is if you flatten the curve, you also prolong, to widen it, and it takes more time. And I don’t see a good reason for a respiratory disease to stay in the population longer than necessary…”[vi]
Stated differently: Flattening the curve with NPI when and where hospitals are not at risk of being overwhelmed is putting off the inevitable and putting the vulnerable more at risk. As it turned out,[2] flattening the curve in most places wasted the opportunity to achieve herd immunity sooner. (For example, Sweden, which had relatively mild NPI, appears to be closer to herd immunity than other industrialized countries.[vii]) Social distancing by young healthy people has similar effects, but its tradeoffs are not quite as negative. For very old people and people with problematic preexisting conditions, social distancing likely remains a prudent course.
Mainstream messaging has been illogical concerning herd immunity. For example, when the mainstream media asks, “Sweden And Herd Immunity: Simple Math Or Plain Madness?” it does not provide an answer. It merely mentions a large number of deaths that might ensue and says something like:
Set aside the fact that, based on recent studies and models, the 1% estimate is wildly too high. Focus on how the 60,000 deaths say nothing about the effectiveness of Sweden’s approach. The real issue concerning total deaths is: Will the ultimate death toll at the end of the pandemic be higher or lower with aggressive this NPI, that NPI, or no NPI? The above media “argument” for aggressive NPI ignores the possibility that Sweden’s ultimate COVID-19 mortality rate could be among the lowest in the world. Why? NPI is designed to manage the wave, not the ultimate number of deaths. Judging a country’s NPI regime when less than 10% of the country’s population has been infected is like taking a snapshot of a horse race before the first turn is reached. Well-respected epidemiologists believe that all the “horses” will “cross the finish line” in a fairly tight pack, i.e., differences in aggressiveness of NPI will have little impact on the ultimate number of deaths in a country.[viii] Worse, comparing the death rates of countries with very different percentages of immune people is either fear-mongering or ridiculous.
Easing NPI in a way that facilitates the invulnerable ninety-plus percent of the population contracting the virus would not be a perfect approach to the problem. No approach to COVID-19 damage mitigation will be. But no one knows that such a policy is not the best available and many epidemiologists believe that it is. Moreover, it is not as reckless as many believe. For the tiny fraction of young and healthy people who have severe symptoms, aggressive NPI will not necessarily save them and it will hurt them.[ix] If people are to get infected, it is likely best to get those problems behind them while the economy is relatively shut down than after they are back at work. In addition, those young and healthy people who are ultra-vulnerable to COVID-19 are extra susceptible to being adversely affected by the virus in any event.
Having the presence of mind to know at every instant what you must do to follow NPI (e.g., never absent-mindedly touch your face between hand washing) is nearly impossible. Can everyone stay 6’ apart from others everywhere and always? They will need eyes in the back of their heads and be quick. We must touch things that may be infected with COVID-9. For example, are you sure no one touched or coughed on your car door handle while you were in the store? Over an extended period of attempts to disinfect, spots teeming with COVID-19 will inevitably be missed. In short, the odds that people can avoid contact with COVID-19, are practically zero. (Cuomo’s chart bears this out.)
We are serious when we say “we must protect the vulnerable.” But, between now and when a vaccine can be deployed, vulnerable people in nursing homes and elsewhere will need multiple shifts of attendants, and contact with nurses, doctors, food and supply vendors, administrators, security people, maintenance people, repairmen, and others frequently entering the complex. If any of them are infected, the virus is on the inside. People inside will receive food, mail, supplies, and other items that may have COVID-19 on the outside of the package or on its contents. The odds that all of those people and materials will be 100% COVID-19-free 100% of the time is zero. Proof of this is born out by the statics that is coming in from around the world showing that nursing homes are often not able to keep the virus out. As Professor Johan Giesecke, MD, Ph.D. said about nursing homes, “We all fail…everywhere in Europe.”[x]
As illustrated in Cuomo’s chart above, a similar, if not worse story applies to people “sheltering” at home. In short, time is not on the side of vulnerable people. The longer we go without herd immunity, the greater the odds that COVID-19 will find its way to venerable people. As more and more people become infected, the more those odds favor the vulnerable. With herd immunity being the only way to stop the virus, the sooner herd immunity is reached, the better.
The mainstream messaging on infections is that more infections are bad. That bad messaging is a huge problem as states start easing NPI. Easing will cause COVID-19 infections to rise for a while. The mainstream response that the rising infection rate is proof that the NPI easing was a mistake is the opposite of the truth and highly counterproductive. So long as hotspots are managed so as to prevent overwhelmed hospitals, many benefits will flow from a rising infection rate. Among the benefits are increasing protection for the sheltered vulnerable and, if the messaging is done correctly, faster economic improvement. Serendipitously, human health concerning non-COVID ailments and human flourishing will improve as well.
The herd immunity messaging problem is that the mainstream media can, and probably will unnecessarily and tragically continue to misinform, confuse, and scare people with negligible risk of harm from the virus into staying at home. Let’s do what we can to help the vulnerable by changing that narrative.
🙛
Caveat Emptor. I feel compelled to repeat, the above observations and claims are not made by an epidemiologist, virologist, or statistician. Therefore, they may be wrong. However, if they are wrong, it is incumbent on those who are “informing” the public to explain why these logical extensions of what is being said are wrong. Otherwise, we will all reap the calamitous harvest of the confusion they are sowing.
UPDATE: During an interview with Mark Levin, Yale’s Dr. Katz captured susinctly the essential point of this post: “The Fauci and Birx practice of flattening the curve doesn’t stop people from dying, it simply changes the date of their death.”
___________________________________ [1] Generally, viruses require between 50% and 80% of the population to be infected, but no one can know the percentage necessary for COVID-19 to fade away to insignificance.
[2] I’m not faulting lockdown decisions made in a panic with little information, much of which was bad. All decisions are made without all the knowledge one would like.
[i] With COVID-19, the death rate is heartbreakingly large and statistically very small. Most who die of COVID-19 had deadly diseases before they were infected. “Nearly All Patients Hospitalized With Covid-19 Had Chronic Health Issues, Study Finds:” “Only 6 percent of patients at one New York area health system had no chronic conditions… [and] and most — 88 percent — had at least two.”
[viii] See link in endnote i. Q: “So you don’t think the severity of these intervening measures are going to make that much difference?” A: “No. I don’t think so.”
As discussed in Part I and Part II of this series, the nonpharmaceutical interventions (“NPI”) deployed in America to fight the pandemic are doing some great good and causing some great harm. The harms include: (1) deaths and a weakening of the immune systems of sheltered people[i] (weakened immune systems open the lid of a pandora’s box of illnesses beyond COVID-19), (2) people have been so frightened by the one-sided messaging about COVID-19 that they choose not to seek needed medical attention, (3) “elective” surgeries to relieve pain and suffering are not being performed, and (4) loss of income, life savings, reserve values of pension plans, and falling home values render buying needed medicines too big a financial risk to take.
A growing chorus of respected epidemiologists says that other than NPIs designed to protect the people in categories known to be especially vulnerable to serious illness or death from the virus (old, infirm, and other specific preconditions), NPIs are doing more harm than good.[iv] Findings like “Experts surprised to find no evidence of COVID-19 spike from Wisconsin’s in-person voting” are mounting. (Can you imagine how dispirited those researchers were?) Protests against NPI, and their irrational/arbitrary rules— abortions are essential but most other “elective” surgeries or procedures, e.g., colonoscopies, are nonessential, and authoritarian enforcement are growing.[v]
In addition to the above, the negatives of: (1) suicides go up one percent for every one percent increase in unemployment,[vi] (2) more deficit spending and creating money/inflation,[vii] (3) normalization of totalitarian style edicts,[viii] (4) mass surveillance,[ix] and (5) people choosing government handouts over jobs[x] have come to the fore. Maintaining currently deployed NPI risks sending the country into an economic death spiral,[1] which, if it happens, will multiply our miseries and deaths.
In short, much misery and death will ensue if the country continues aggressive NPIs, discontinues NPI, or anything in between. If the county’s economy remains too throttled too long, more misery and death will be caused by the throttling than would be caused by COVID-19. Consequently, the current NPI regime must be eased at some point and waiting for a vaccine, which may never come, is untenable in light of the uncertainty and waiting times for a vaccine and the mounting negative consequences of NPI.
The foregoing assumes the economy has not already gone beyond the tipping point. Though it may have, there are good reasons to doubt NPI has already sent the economy into a death spiral. The Spanish flu and its NPIs caused more economic destruction than the COVID-19 virus and its NPIs have caused so far. In terms of life-years lost,[xi] there is and will be little comparison between the Spanish flu and COVID-19. Nevertheless, within two years after the Spanish flu pandemic, the US economy came to be fairly described as “The Roaring Twenties.” During that period, workers’ wages rose significantly and the economy boomed.[xii]v
The above analogy will not apply if the government too actively tries to fix the economy once the NPIs are removed. In 1921 President Coolidge sprang into action to prevent the federal government from much involvement in fixing the economy, and entrepreneurs and workers took it from there.[xiii]
When does “throttled too long” happen? No one does or can know. All of the practically infinite variables affecting that outcome cannot be identified and the identifiable ones that cannot be sufficiently quantified to confidently predict either the time or the conditions that would cause a death spiral. We do know, however, that every minute the economy remains throttled nudges the economy closer to the cliff, and every minute people remain shielded from pathogens and beneficial bacteria and viruses weaken immune systems—thereby rendering Americans more vulnerable to other viruses and bacteria, including possible mutations of COVID-19. As I said, waiting for a vaccine is untenable.
On the other hand, the reopening of businesses will do little good if too few erstwhile customers are willing to engage in enough commerce to keep businesses afloat. Reopened businesses can survive only if enough people believe either that patronizing business is “safe enough” or that they should patronize businesses despite the safety risks.
We’ll sort out both of the above points in upcoming posts.
UPDATE: An important negative consequence of NPI not mentioned in the original post is the fact that people sheltering are in stress. The Mayo Clinic puts it this way: “Chronic stress can wreak havoc on your mind and body.” (Click on the text for details.) Sources of stress are many without a pandemic. To add to those stressors things like sheltering fearing that, at any moment, a family member or one’s seld could contract a horrible, if not deadly, disease is a huge stressor. To add even more to that stress, one sitting at home with little to do leaves lots of time to stress oneself out more by focussing on the problem.
______________________________
[1] The “death spiral” is predicated on the expectation that when business failures cause massive job losses, collapses of 401k, other retirement savings, and pension fund assets, and out-of-work people, including retirees, have insufficient assets with which to buy their necessities, (and ripple effects of all of that), the government will create more money/inflate the currency/reduce confidence in the US dollar, as it tries to sustain a population that does not produce as much as it consumes. Eventually, buyers for US bonds will dry up because of the declining prospects of US bonds being the safest investment in the world. With bond sales being no longer available, the government will have not option but to create more money to fund its unfunded liabilities and desires to spend even more. The consequences of that spiral are hyper-inflation, panic, and the collapse of the economy. Those events will cause civil disruption, further taxing the government and serial decimations of the quality of life, which will span more civil disruption.
[ii] “We Might Never Get a Good Coronavirus Vaccine:” “COVID-19 could be a virus that proves resistant to vaccination. ‘This may be one,’ [Rachel Roper, a professor of immunology at East Carolina University who took part in efforts to develop a SARS vaccine] says. ‘If we have one, this is going to be it, I think.’”
[iii] “Deaths following vaccination: What does the evidence show?” While this article’s title indicates the it will tell the reader how many people are killed by vaccines, the article is mostly about the data that supports the notion that vaccines are a good idea. As true as that may be, the fact that the article doesn’t not say that “the evidence shows” that no people are killed by vaccines (a fact that would be in the opening line of the article if it were true, is not included in the article.
[vi] “Psychology Today,” “Unemployment is a well-established risk factor for suicide. In fact, 1 in 3 people who die by suicide are unemployed at the time of their deaths. For every one-point increase in the unemployment rate, the suicide rate tends to increase .78 points. One of the silent drivers of our current suicide crisis is the high percentage of working-age men not participating in the labor force.” “Dr. Ioannidis on Results of Coronacirus Studies.” @6:35
[xii] “Economic Effects of the 1918 Influenza Pandemic.” “Using state-level personal income estimates for 1919-1921 and 1930, the authors do find a positive and statistically significant relationship between statewide influenza mortality rates and subsequent state per capita income growth… Some academic research suggests that the 1918 influenza pandemic caused a shortage of labor that resulted in higher wages (at least temporarily) for workers…”
The goal of this series of posts is to explore ways to strike a workable balance between the dueling concerns about health and the economy that are raging. We must deal with the Gordian Knot that while businesses need to reopen, reopening businesses is futile if customers are unwilling to engage with the businesses. Let’s lay the groundwork for that discussion by noting how we got to where we are and then sorting out where we are.
To scare people enough to get them to follow NPI suggestions and orders, the government officials, with the aid of experts and the mainstream media, launched a massive and biased publicity campaign using the scariest numbers to which credible academics would affix their names. More honest and realistic messaging, however, likely would not have worked as well in getting people to follow recommendations and orders. Governments must work with the overly fearful[i] and innumerate[1] citizenry they have, not the citizenry they wish they had.
Consequently, a good case can be made that the deceptive and hyperbolic fear campaign was warranted. Bereft of reliable data concerning the virus (other than it was deadly and coming), full of uncertainty as to how Americans would adhere to NPI orders or recommendations, and confronted with the possibility of inestimable horrors, doing nothing would have been untenable in America’s fearful and disunited society. The campaign met its objective of preventing hospitals from being overwhelmed—even in the hardest-hit New York City. Achieving that objective likely saved many lives and kept doctors from having to decide who lives and who dies, as was the case in Italy. (The NPIs have and will continue to cause deaths as well, but whether the lives taken by the NPIs will exceed the lives saved by the NPIs is academic at this point.)
The stated objective of the NPIs was to “flatten the curve” (slow the pace of infections) so (1) hospitals would not be overwhelmed, (2) the number of people infected during the winter would be reduced (in hopes that warmer summer weather would suppress the virus while scientists gathered and analyzed data to device more informed strategies to deal with the virus when as it spreads across the population). Note, however, that flattening the curve had mostly to do with when the maximum number of people would get infected, not if. It was and is assumed that the virus will continue to spread across the population until enough people are infected to achieve herd immunity. Although one should acknowledge that NPIs might cause there to be fewer deaths if treatments and devices are found to lessen the severity of illnesses and/or reduce its mortality. While the need to get started on vaccines was a topic of conversation, virtually, no one expressed confidence that a vaccine would be invented, tested, approved, and administered within a year, and experts knew that a vaccine might not happen.[ii]
As discussed in Part I, sheltering in place waiting on a vaccine to save the day wasn’t, isn’t, and won’t be a sound strategy. On the contrary, among other things, doing so would cause many illnesses, financial ruin, spousal and child abuse, and deaths. A very relevant example is that people who shield themselves from viruses and bacteria are weakening their immune systems, i.e., making themselves more vulnerable to illnesses[iii] and not doing their part to achieve herd immunity for many diseases, including the possible winter wave of COVID-19.[2]
Looking at vaccines in the context of “herd immunity” is essential. Is herd immunity a big deal? Yes:
“With all respiratory diseases, the only thing that stops the disease is herd immunity. About 80% of the people need to have had contact with the virus…”[iv]
According to theory, vaccines are a relatively low-risk way to help achieve herd immunity. However, in terms of the health and wealth of a population, the sooner the herd immunity exists, the better. Given that, if there are other low-risk ways to reach herd immunity, waiting for anything, including a vaccine, is a bad idea. That would be true even if there were no high costs inflicted by imposing NPI on people who, with very little risk, could help gain herd immunity sooner, be more productive, enjoy camaraderie, and have more fun. As discussed above, however, being isolated in a relatively sterile lonely house, however, does inflict high costs.
While herd immunity is the best weapon available to defeat COVID-19,[v] consider these important facts about herd immunity:
For the pandemic to be put to rest, from 50%[vi] to 80% of the population will need to have been infected,
The sooner a herd immunity level of infections is achieved, the sooner it will be reasonably safe for vulnerable people to get back out into the world and enjoying their lives,[2] and
By staying at home, people who have a tiny chance[vii] of having severe effects from a COVID-19 are unnecessarily delaying the process of both getting on with their lives, getting the economy back on track, and getting the pandemic behind us—provided the exceptionally vulnerable continue to follow NPI practices until it is reasonably safe to do so.
Given that the goal is to achieve herd immunity, the longer most people stay at home, the more slowly the country will reach “herd immunity,” which, save a miracle, is the ultimate goal of all efforts to deal with the pandemic. It stands to reason that the likelihood of being infected decreases as the percentage of infections increases, i.e., the benefits from more people being infected begin before herd immunity is reached.
So how do we cause young healthy people comfortable enough to engage in commerce? We’ll begin sorting that out in Part III of this series.
____________________________________
[1] If one does not understand the concept of odds or is not proficient in its application, one can have no clue what to make of risks. Stupidly avoiding small risks and stupidly taking large risks are both counterproductive and dumb. Suffering from innumeracy results in dangerous mistakes and causes people to favor foolish government policies.
[2] People who are exceptionally venerable COVID-19 should not be expected to expose themselves to exceptionally dangerous risks, including exposure to the herd.